InvoiceWriter
LOGIN
SIGN-UP
- Invoice Generator
doctor
medical
insurance
physician
dr.
hospital
clinic
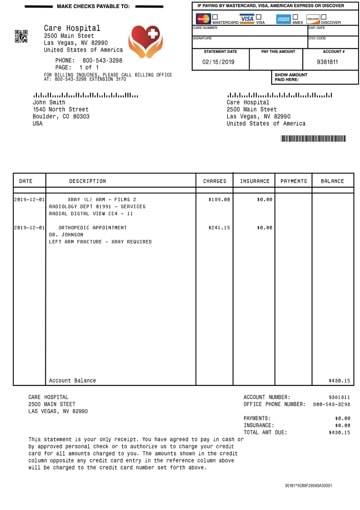
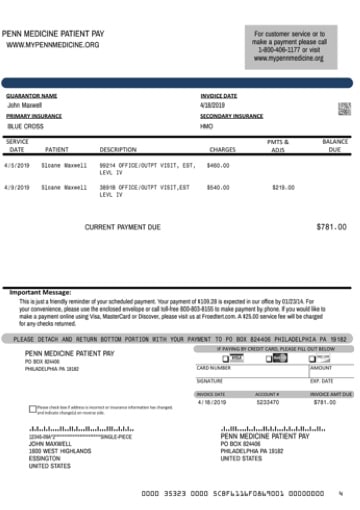
Use this generator below to create an invoice that will be exact replica of a .
Create authentic looking receipt / invoice by entering data and clicking "Preview" button.
Fill Sample Data
Email
Download
Preview
Edit
Business Name
Business Address
Business City, State Zip
Business Country
Business Telephone
Business Website
Customer Name
Customer Address
Customer City, State Zip
Customer Country
Customer Telephone
Account #
Service Date
Invoice Date
Due Date
Payment
Payment
CASH
VISA
MC
AMEX
CARD
DEBIT
CHECK
Primary Insurance
Secondary Insurance
Patient Name
Browse
DATE
DESCRIPTION
CHARGES
INSURANCE
PAYMENT
+
New item
CURRENCY
$
€
£
¥
Rs
Notes
Looking for MORE invoice templates? Try
PDF Pro - Invoice and Receipt Creator
Related Invoices
Related